
Medicaid, the combined federal-state health insurance program for disabled and low-income people, was long considered low-quality, and was associated with a cultural stigma as a government handout benefiting poor, broke or lazy people.
But thanks in part to the Affordable Care Act, the program is shedding that association. Medicaid now covers more people than ever and many enrollees say they are satisfied with the quality of care and the ease of applying, and they feel less shame using the program.
For this article, we talked to experts and Medicaid enrollees about their experiences and about changing perceptions.
She lost her job and her health insurance
When Julie lost her job last year, she dreaded losing her health insurance. (She spoke on condition that we use only her first name to protect her privacy.) She suffers from a chronic health problem and her COBRA payments for extended insurance would have been astronomical. And she thought she would have to pay big money on the Obamacare marketplace for a high-deductible plan.
But when Julie found out she might qualify for public health insurance, she was relieved but also dubious. She filled out the income and family size questionnaires on the health exchange for the state she lives in, truthfully, including her current lack of income, and the result surprised her.
“I was being considered for Medicaid,” Julie said in a phone interview. “And I was like, I don’t know how to feel about this.”
Julie’s experience is not rare. For decades after its inception, Medicaid was widely considered a low-quality offering.
But thanks in part to the Affordable Care Act, the program is shedding that association. Medicaid now covers more people than ever and many enrollees – 84% in states that expanded Medicaid under the Affordable Care Act and over 90% of parents nationwide whose children are in the children’s version – say they are satisfied with the quality of care and the ease of applying, and they feel less shame using the program.
Medicaid was first signed into law by President Lyndon Johnson in 1965 as a health coverage program for people with disabilities who could not get insurance through employers. It was later expanded to cover people with low incomes in general.
Longstanding stigma
Dr. Heidi Allen, an associate dean, professor and researcher at the Columbia University School of Social Work who studies Medicaid, said it became associated with poverty, and the culture and the medical establishment came to regard the coverage as cheap and the recipients as grifters.
“There are all sorts of layers to stigma,” she said. “Stigma can be public perception of a program. It can be provider experience of a program, provider experience, and stereotyping of patients who use a program.”
This rang true for Julie, who felt like she didn’t fit the stereotype of a Medicaid user.
“I’m pretty sure I have some extended family members, who would just be beside themselves if they knew that I was on Medicaid,” she said. “Because they would be thinking that I have more earning potential and I shouldn’t be like taking away services from people who really need them.”
Providers’ attitudes toward Medicaid
Allen has also found that medical providers project stigma onto their Medicaid patients. Her 2014 study looked at a cohort of Oregon residents on Medicaid and found that a significant number of people felt stigmatized by the medical establishment. (Because Medicaid is a joint state-federal program, generalizations to the entire United States population and its relationship to Medicaid is difficult, and it is entirely possible that if her 2014 study were repeated today, the results – post-Recession, and given the effects of the pandemic and its job losses and economic effects – would be different.)
Medicaid does pay doctors less than many private plans, so many high-earning doctors won’t accept it. But that doesn’t account for why people look down on the recipients.
“Our system is set up based on categories that people fit into. And those categories are hierarchical, in, you know, some unspoken measure of worthiness,” Allen said.
If that stigma leads to patients avoiding care, that can lead to worse health outcomes.
A cultural shift on Medicaid use
Yet the biases about Medicaid may be becoming less powerful and less prevalent, at least for some if not all people.
Hailey, a college student in Virginia who also works part-time in the restaurant business, enrolled in Medicaid as soon as she turned 18 and aged out of her mother’s Medicaid plan.
“I never felt a social stigma about it,” Hailey, 19, said in a phone interview. (She also spoke on condition that only her first name be used.) “I never felt shame using Medicaid.”
She is part of a younger generation and, unlike Julie, had never conceived that others might think she’s irresponsible by using Medicaid.
“Honestly, if you’re 18 years old and you’re getting Medicaid, you’re actually being extremely responsible,” she said. “Most 18-year-olds might just say, ‘Oh, I don’t need insurance.’”
Dr. Martha Livingston, professor of public health at SUNY Old Westbury who studies policy and social factors of healthcare, said most of her college-age students are openly on Medicaid.
“I have plenty of students whose families are on Medicaid,” she said.
And she finds that it’s not only young adults who are satisfied and free of stigma.
“I have not personally experienced anybody feeling any kind of shame, about accessing their care through Medicaid.”
Affordable Care Act effects
Experts say it was the Affordable Care Act, the landmark healthcare package enacted by President Barack Obama in 2010, that is responsible for this sea change. The new law offered billions of dollars in federal money to any states that opted to expand their Medicaid programs, offering benefits to a wider population of its uninsured residents. While not all states opted to increase their rolls, 39 states and Washington, D.C. did offer Medicaid to more residents resulting in a nationwide surge of over 21 million more Americans getting healthcare through the program.
The government said that as of November 2022, 91.7 million Americans are now covered by Medicaid, including its sister public insurance plan, Children’s Health Insurance Program. That’s 19% of the country, making it the largest insurer in the U.S.
One big part of the Medicaid story is the Children’s Health Insurance Program (CHIP). It predated the A.C.A.; the CHIP Reauthorization Act (CHIPRA) reauthorized CHIP in April 2009 and the A.C.A. contained provisions to strengthen the program. It has since been expanded to include more children. CHIP, a subset of Medicaid for children, also requires means testing (household income and family size must be reported) yet it encompasses a large number of children.
“Of the 8.6 million children in working families who are covered by public insurance, more than 70% have a parent who works at a large, private company, according to a new study from PolicyLab at Children’s Hospital of Philadelphia,” WUSF Public radio reported in 2019. Many of those families, then, have parents covered by company insurance and children on CHIP.
But higher numbers alone don’t explain a lessening of social bias. The key, Allen said, is that we all know someone on Medicaid, so it’s harder for us all to maintain our old, stereotypical ideas of a Medicaid recipient.
“You’re more likely to know somebody who is on Medicaid or benefited from Medicaid. In the years since the Affordable Care Act passed,” Allen said.
Also, the average Medicaid enrollee is less likely to be poor, since many states stopped limiting the program to people who live below the poverty line and began offering it to people who earn a little bit more than that as well as people who are between jobs.
Julie said a close friend said “‘I was on Medicaid, when I had that big gap between jobs, and it was great,’” Julie said. “She also had a really positive experience with it.”
Medicaid enrollees are generally happy with their coverage
Also contrary to what you might think, in many states, the quality and quantity of healthcare Medicaid enrollees are able to access is pretty good.
Julie heard from her mother that Medicaid was actually considered good insurance by many people in New York.
“She was like, oh, ‘Medicaid is the best insurance. If you can, you should absolutely do it,’” she said.
To be sure, more doctors accept private insurance than Medicaid. Physicians who don’t take Medicaid cite not only lower pay rates than private insurance – even lower than its sister program, Medicare – but also a higher rate of claim denials and the administrative burden, hoops they have to jump through to submit bills for payment.
While numbers vary by state and by physician specialty, a nationwide study carried out by the Department of Health and Human Services found that a large majority of doctors were accepting new Medicaid patients: 68.9%, while 84.7% doctors were accepting private insurance. (Of course, a doctor may “accept new Medicaid patients” but have appointments only months and months away, or at an inconvenient time or location, limiting patient loads in that way while publicly saying they are accepting patients.) Private insurance plans available on the A.C.A. marketplace or through your employer generally have 10% to 70% of providers in a given region accepting their plans, but these provider lists are widely known to be wildly inaccurate, and there have been frequent reports recently that doctors say they are accepting new patients while in truth they have few or no appointments.
States that did not expand Medicaid
It is also true that there are a number of states where the governor and the legislature refused to expand Medicaid, even with the infusion of federal money. In those states, Medicaid seems to be more limited (to only the poorest of the poor) and also to have fewer providers. Georgia comes up a lot in this context, but North and South Carolina, Tennessee, Mississippi, Alabama, Florida, Texas, as well as Kansas, Wyoming and Wisconsin did not expand Medicaid under the A.C.A.
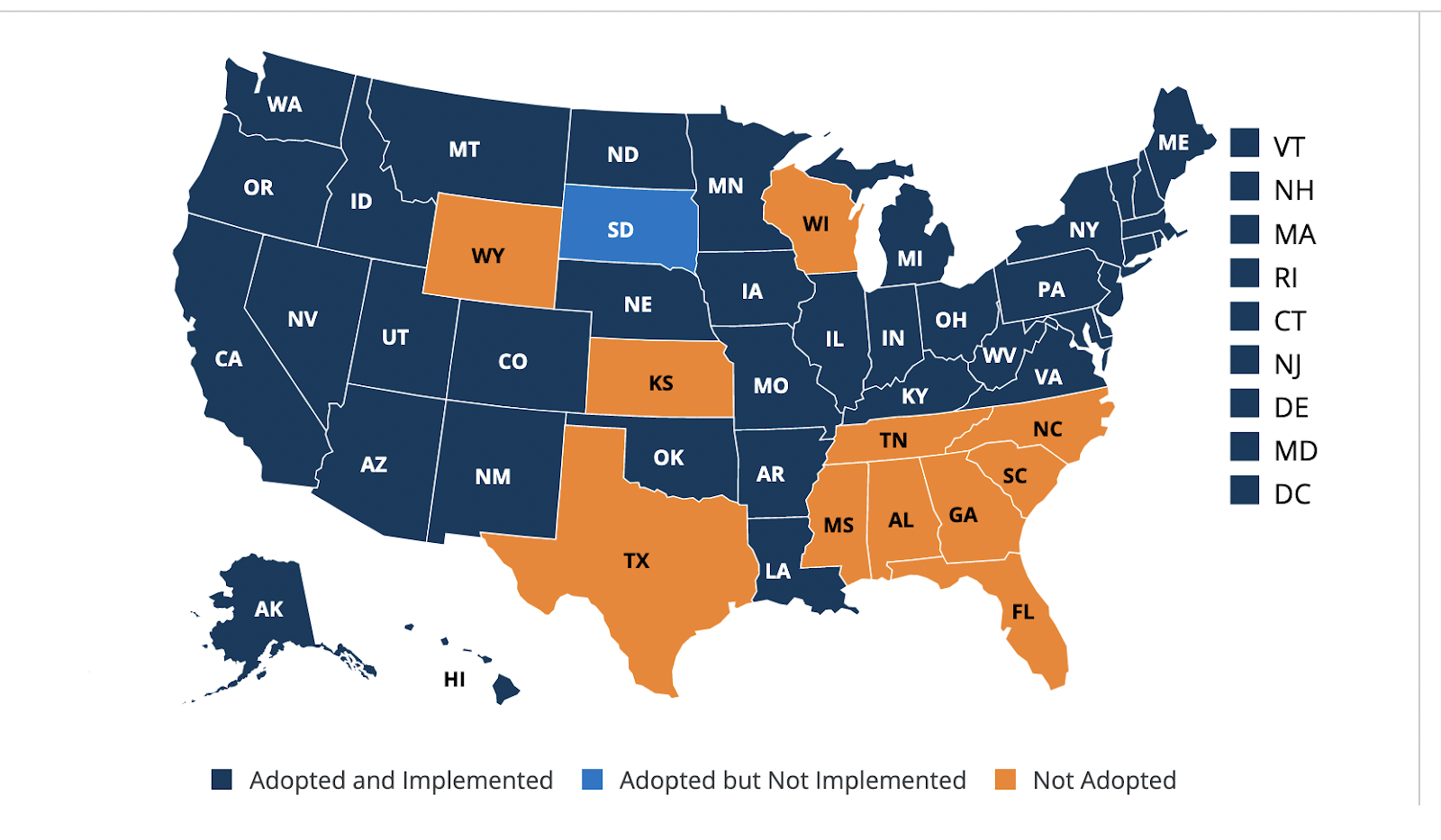
(Source: Kaiser Family Foundation, February, 2023)
A number of other states have instituted work requirements for those on Medicaid, and for them continued enrollment may be precarious.
Again, coverage varies widely by state but finding a provider is sometimes just the luck of the draw and timing – with any insurance plan.
“[Before selecting a Medicaid plan,] I called several of my doctors to ask them if they take a Medicaid plan? If so, which ones?,” Julie said.
Julie’s path sounded like the path of anyone switching insurance, private or public – not necessarily simple.
“I’m someone who likes to really analyze things,” she said. “And I happen to go see a lot of doctors.”
Julie said she spent about a day and a half on the phone with doctors and New York’s department of health trying to figure out which of the plans was best for her.
Hailey’s experience in Virginia wasn’t as positive, but she still thinks being on Medicaid was better than the private coverage she had to buy on the marketplace once she began working.
“Trying to find a doctor wasn’t always the easiest, because you have to call [so many] different places. Especially when it was a specialist. In the end, I couldn’t go get a second opinion, because there was only one that took Medicaid, it was super far away,” she said. “[Medicaid] was really helpful. Now that I don’t have it, I realized that I could just go to a doctor when I needed to.”
What you can do
Find out if you qualify: Medicaid and CHIP are both means-tested, meaning you may qualify if your income is low enough. Many people are surprised they are eligible for the benefits. This is particularly true for CHIP; in one family we learned of, neither parent qualified for Medicaid and one child was on a student health plan. The second child, who had multiple health issues, qualified for CHIP, surprising his parents – but they were very grateful when his health issues landed him in the hospital several times.
How to pick a health insurance plan: In most states, Medicaid benefits are administered through private companies – managed care organizations – just like Medicare and private insurance. You’ll have to choose which plan best meets your needs.
You can search by county in New York for the ones that operate in your area and then look into which providers participate in your network. New York City, for example, has about a dozen options. The city’s Department of Social Services published this guide to choosing a plan with tips including: Ask the doctor you regularly see for the names of the Medicaid plans that she or he accepts; look at the plan’s network to see if the doctors, hospitals, and clinics are close to you and check to see if the health plan covers your medications.
Find a doctor that accepts Medicare or Medicaid: The U.S. Department of Health and Human Services provides this online tool for finding providers. We tried it and found it’s not always accurate. Calling your state’s health department may be more efficient.