
The drug Humira is the world’s biggest medication moneymaker: It brought in more than $15.6 billion in the first 9 months of 2022 for its manufacturer, AbbVie. Now it’s coming off patent and losing its exclusive hold on the market – and its manufacturer wants to keep making money, as the drug gains competitors that cost a fraction of the price.
So Humira is a fascinating way to look at drug pricing in the United States — and also to ask whether patients will actually save money now that there is a generic.
Humira (generic adalimumab) is used to treat inflammatory conditions like rheumatoid arthritis, psoriatic arthritis, Crohn’s disease, ulcerative colitis, ankylosing spondylitis and psoriasis. Patients inject it themselves, and it is one of the widest-used and most expensive medications on the market. The cost for patient and insurer is often more than $80,000 annually.
Why is it so interesting? “Humira is at the epicenter of so many earthquakes that are rocking the healthcare system,” said Robin Feldman, distinguished professor of law and head of the Center for Innovation at the University of California College of the Law, San Francisco.
“Humira is a widely used drug with sky-high prices. It is also a biologic drug” – a class of drugs made by using a living organism or its products, she said. “And much of the industry is rushing towards developing biologics these days – in part because, for successful drugs, the profit margins are so high. With Humira, the company has thrown curveball after curveball at potential competitors.”
Now, despite AbbVie’s strategy to squelch competitors, they are here. Feldman said, “The name of the game is how do you keep competitors out? Humira cannot block them completely, so how do you limit them?”
One answer: The middlemen
The complex nature of the market, giving huge power to the middlemen, known as pharmacy benefit managers (P.B.M.’s) is at work here, she said.
“In the U.S. reimbursement system, P.B.M.’s. negotiate prices with drug companies, and they decide whether the patient will be reimbursed and the terms on which the patient is being reimbursed. They direct the prescription flow of patients. They channel patients into higher-priced drugs and away from less expensive drugs. That’s how they get paid more.”
So the next steps for the non-Humira competitors, she said, “are all about dealflow from the middle players.” AbbVie cannot block competitors completely, so how can it limit them?
When pharmacy benefit managers arose in the late 1960’s, the idea was that they would help insurers save money, specializing in drug supplies and pricing while insurers concentrated on doctor’s appointments, hip replacements and so on. But the P.B.M.’s began to take on other roles: They buy medications, set prices, negotiate rebates (discounts paid by a manufacturer to a P.B.M.), set formularies (lists of preferred medications, often based on pricing), process claims, review and assess drug use, and so on. They essentially set the price people pay for medications by arranging all these things behind the scenes.
The three largest – Express Scripts (owned by Cigna); CVS Caremark (a subsidiary of the CVS drugstore chain), and OptumRx (the pharmacy service segment of UnitedHealth Group Insurance) – control approximately 89% of the market, according to the National Association of Insurance Commissioners.
Those P.B.M.’s steer patients to their preferred or wholly owned pharmacies (CVS) and away from independent pharmacies. They also are huge drivers of their parent companies’ profits.
“More than half (52%) of three companies’ profits in 2022 came from their PBM business units: Cigna’s Evernorth, CVS/Aetna’s Caremark, and UnitedHealth’s Optum. Cigna now gets far more revenue and profits from its P.B.M. than from its health plans. And CVS gets more revenue from its P.B.M. than from either Aetna’s health plans or its nearly 10,000 retail stores,” Wendell Potter, a former Cigna executive who now is a health system critic, wrote on his Substack.
The Federal Trade Commission and the House Oversight and Accountability Committee have launched investigations into the pharmacy benefit managers.
How a rebate works
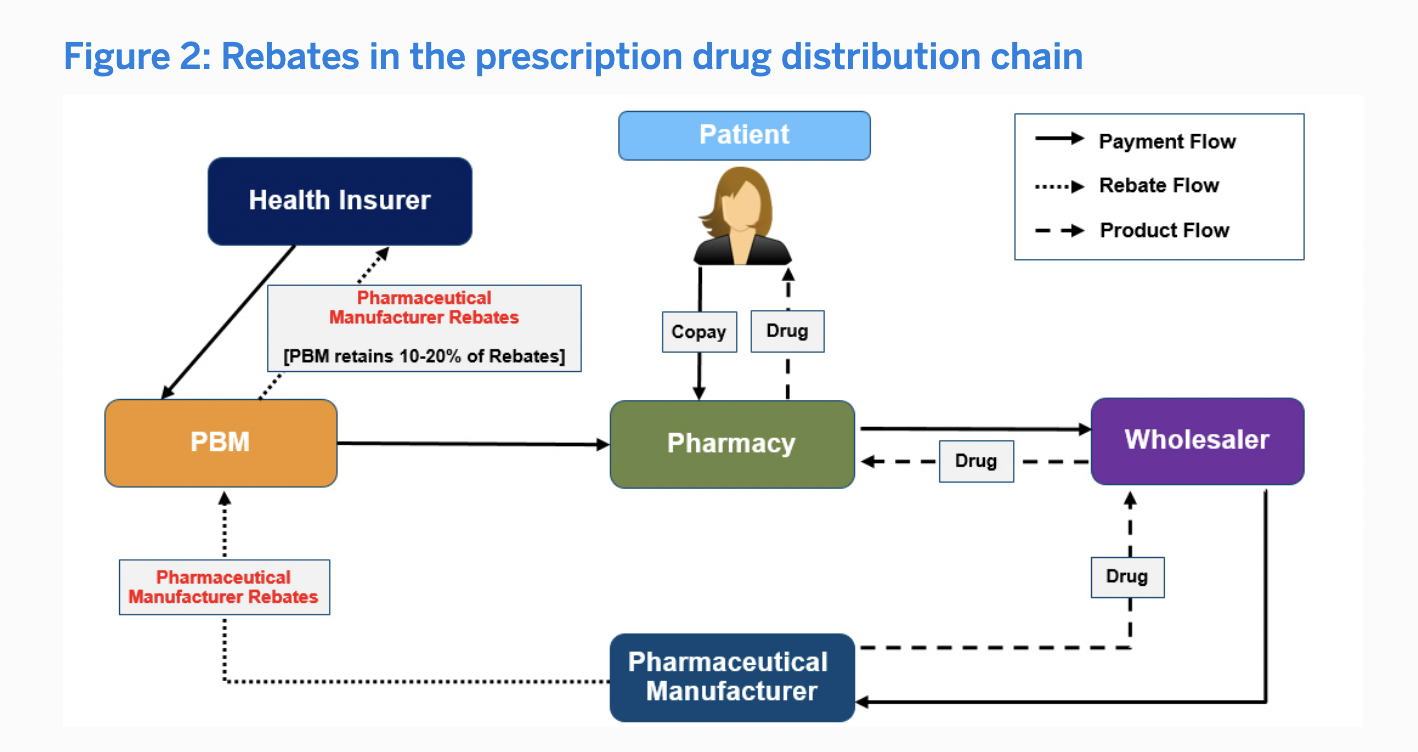
The system as it currently operates, Feldman explained, rewards all the players for increasing the price of a drug so the middlemen can collect money in the form of rebates, administrative fees and so on.
“A variety of middle players want those extra dollars,” she said. “With lower prices, you don’t have the extra dollars for the middle players, and the middle players won’t direct patient care. All of this is completely perverse. As one doctor said, and I quote, ‘It’s Alice in Wonderland in the medical industry,’ and I like to add, ‘Yes, and it’s our dollars going down the rabbit hole.’”
To understand this, it makes sense to know how a patient pays for a medication. She goes to the pharmacy and wants her drugs to be “covered,” a perfectly understandable desire from an insured person.
If the patient uses the “preferred” drug, she will supposedly pay less, in the form of a lower copay or lower co-insurance, Feldman said. “The system is supposed to direct patients to drugs that are less expensive and just as effective,” she said. “But the system has been manipulated.”
“That’s the problem that we have now. This reimbursement system was originally designed to save money. But it’s been completely diverted in the interest of all the parties along the chain for their own interests, not the patient’s interests,” she said, and now all the forces along the supply chain conspire to increase prices, instead of reducing them.
Why don’t prices go down?
The forces driving prices up here are similar to those elsewhere in healthcare.
For one thing, a lot of payments for P.B.M.’s come in the form of “administrative fees” – often based on the percentage of a total bill. An administrative fee for a $1,000 drug is bigger than on a $10 drug, so the pressure is for prices to go up.
A second reason: The middle players figure their rebate on the price of the drug. “How do you generate a bigger rebate?” Feldman said. “You have to raise the price of the drug so you can bring it back down.”
It’s like a coat store raising the price of a jacket before putting it on sale, she said: “It looks like a good price, but it isn’t.”
Then once the higher price is established as the sticker price, some people will have to pay it – people on high-deductible plans, for example.
“The sticker price is rising faster than the rebates are,” she said. “It’s like buying the same jacket, but paying more and more over time. And those are only two of the ways that middle players get paid.”
A third way, she said, is that some contracts between middle players and health plans are based on the size of the rebate they finally negotiate.
“So how do you get a higher rebate? You have to get the pharma company to raise the sticker price, so you can show you have negotiated a bigger rebate.
“At the end of the day, the system drives prices higher, and channels patients toward more expensive drugs.”
The sticker prices are rising faster than the rebates are, she said: “You are buying the same jacket, but paying more and more over time.”
(To understand more about rebates, read this Milliman white paper, the source of the diagram reproduced here.)
This has all been going on for many years, she said. “If my job is to lower prices, and after 15 years prices on the same drugs have gone up 300%, I’m not doing a very good job,” she said. “That’s how that’s how the system is working.”
Pharmacy benefit managers make money in other ways too – for example the hard-to-understand D.I.R. fee. In describing this, RXSafe, a supplier of pharmacy automation technology, writes: “Direct and indirect remuneration” fees are imposed on pharmacies after a patient sale that is not readily predictable. These fees may include ‘pay-to-play’ fees for network participation, periodic reimburse-reconciliations, or non-compliance with quality measures.”
If you’re not confused yet, don’t worry – there’s still more opportunity: at a conference I attended once, a speaker for a small drug middleman said she had counted 32 different ways that P.B.M.’s make money.
The patent system
One other factor pushing the prices up is the drug patent system, Feldman said. Drug patents are designed to provide “a time-limited opportunity for companies to make a handsome return, then they are supposed to go back to the lab and invent new things,” Feldman said. But the end of life of a blockbuster patent “is a terrifying time for a company,” so companies look for ways to extend the monopoly, she said.
AbbVie competitors have sought to create biosimilars – drugs that are competitors to drugs like Humira, created inside of living cells. Unlike generics, biosimilars are not identical, and so they cannot be automatically substituted for a medication like Humira.
What AbbVie did to protect its market position was to take out a ton of patents and then sue any potential competitors.
“AbbVie and its affiliates have applied for 311 patents, of which 165 have been granted, related to Humira, according to the Initiative for Medicines, Access and Knowledge, which tracks drug patents,” The New York Times reported in January. “A vast majority were filed after Humira was on the market.
Some of Humira’s patents covered innovations that benefited patients, like a formulation of the drug that reduced the pain from injections. But many of them simply elaborated on previous patents.
“For example, an early Humira patent, which expired in 2016, claimed that the drug could treat a condition known as ankylosing spondylitis, a type of arthritis that causes inflammation in the joints, among other diseases. In 2014, AbbVie applied for another patent for a method of treating ankylosing spondylitis with a specific dosing of 40 milligrams of Humira. The application was approved, adding 11 years of patent protection beyond 2016.
“In 2016, with Amgen’s copycat product on the verge of winning regulatory approval, AbbVie sued Amgen, alleging that it was violating 10 of its patents. Amgen argued that most of AbbVie’s patents were invalid, but the two sides reached a settlement in which Amgen agreed not to begin selling its drug until 2023.”
The Times reported that AbbVie reached similar agreements with nine other manufacturers, who all agreed to delay entry into the market until 2023 – so AbbVie competitors agreed to wait, apparently because the payoff was big enough.
Patient assistance programs
Of course, it’s true that a patient assistance program may help patients get Humira at a reduced price. Many drug companies have patient assistance programs, which grant price breaks; the patient must find the plan and then apply for it. (Google “patient assistance plans drugname.)
The savings can be tremendous: We have heard of patients getting their medications for $5 a month, for example.
With all such plans, there can be limits and loopholes. Most will not allow anyone using public insurance plans (Medicare, Medicaid, Tricare) to use them. There are often cumbersome requirements – a 6-month time limit, a lifetime cap, a dollar limit. Some require you to use your health insurance to pay a portion of the cost.
With patient assistance programs, the big drug companies write off the sums ascribed to the plan on their taxes. And the companies, when confronted with a high drug price, can say “That’s why we have a patient assistance plan.” Read more at our “how to save money on prescriptions” post.
So now it’s 2023: what’s happening with prices?
One of the first things to happen: Amgen released its biosimilar, Amjevita, at two different prices, one 55% below Humira’s list price and the other at 5% below Will this save patients money? Maybe not.
An analysis of the market by Goodroot suggests that AbbVie will try to maintain its market share by increasing rebates, so the middlemen will not have an incentive to switch. ”If they increase their rebate, it will be nearly impossible for biosimilars to make the cost impact that many are hopeful for,” Dermatology Times wrote.
So if the P.B.M. keeps Humira on the insurance formulary — the list of approved drugs — because it’s getting a nice rebate, will patients be able to switch without paying out of pocket?
“Still to come later this year are Humira biosimilars from Boehringer Ingelheim, Novartis’ Sandoz, Organon, Pfizer, Mylan, Coherus and Fresenius Kabi.” Fierce Healthcare reported.
What’s next?
What can a patient do? Or will regulatory approaches or other approaches change the picture?
Feldman pointed to two disruptive examples in the marketplace.
One is Mark Cuban Cost Plus Drugs, the company funded by the zillionaire executive that is a generics-only source for medications: Prescriptions can be bought for the cost of manufacturing plus a 15 percent markup, and an additional fee for mailing, the site says.
Mark Cuban Cost Plus is starting to sell a biosimilar to Humira this month, at a price of $584.27 for a box of two autoinjectors, as opposed to $6,992 for the AbbVie version. Of course with Mark Cuban Cost Plus, the price is cash; any insurance benefit is up to the patient to find.
I myself have used Mark Cuban Cost Plus and saved a bunch. The company does not have every generic, and it’s still not widely known. Also while I am saving money by going this route, it would be better – to my mind – that Medicare and my Part D insurance company, Aetna, would stop playing the game that makes me pay more for my medications by paying cash than by using my Medicare Part D insurance card through Aetna.
In one case, Mark Cuban charged $10 a month for a medication my drugstore wanted to charge $68 for under insurance. In another, Mark Cuban charged $18.20 for a medication my drugstore was selling for $76.20.
Feldman said another disruptive move in the market is the stated aim of the state of California to make its own generic insulin and sell it at a very low price. This does not apply to Humira right now, but it is possible to see from here how California might decide that if it succeeds with insulin, it will do the same thing with Humira.
Doctors, medical choices and money
One other thing will not be affected. Doctors often want to keep patients on a medication that is working for them. From a patient’s perspective, that can be a very good thing: There is ample evidence that not all generics work the same as all brand-name medications. So switching to a generic might not happen, or might not happen easily.
Beyond that, AbbVie consistently pays a lot of money to doctors, hospitals and other providers.
Don’t forget — this kind of payment to doctors is completely legal, for consulting, promotional talks, meals and more. It is something that a drug company considers part of the cost of doing business. And ProPublica, the investigative newsroom, found that the more money the doctor gets from a drug company, the more likely she is to prescribe that company’s drug.
This page on the openpaymentsdata.cms.gov website documents AbbVie’s generous payments to doctors, hospitals and others. Montefiore Medical Center, just one town over from me, is a primary recipient, as is the University of Washington — and several individual providers. In 2022 alone, AbbVie reported paying over $53 million in “compensation for services other than consulting, including serving as faculty or as a speaker at a venue other than a continuing education program” and over $28 million in food and beverage payments.
Of course, not all of these payments are related to Humira — AbbVie has a number of products — but it’s certainly worth considering if a doctor who got lots of consulting fees from Abbvie will prescribe a lot of Humira.

Abbvie openpaymentsdata.cms.gov payments.
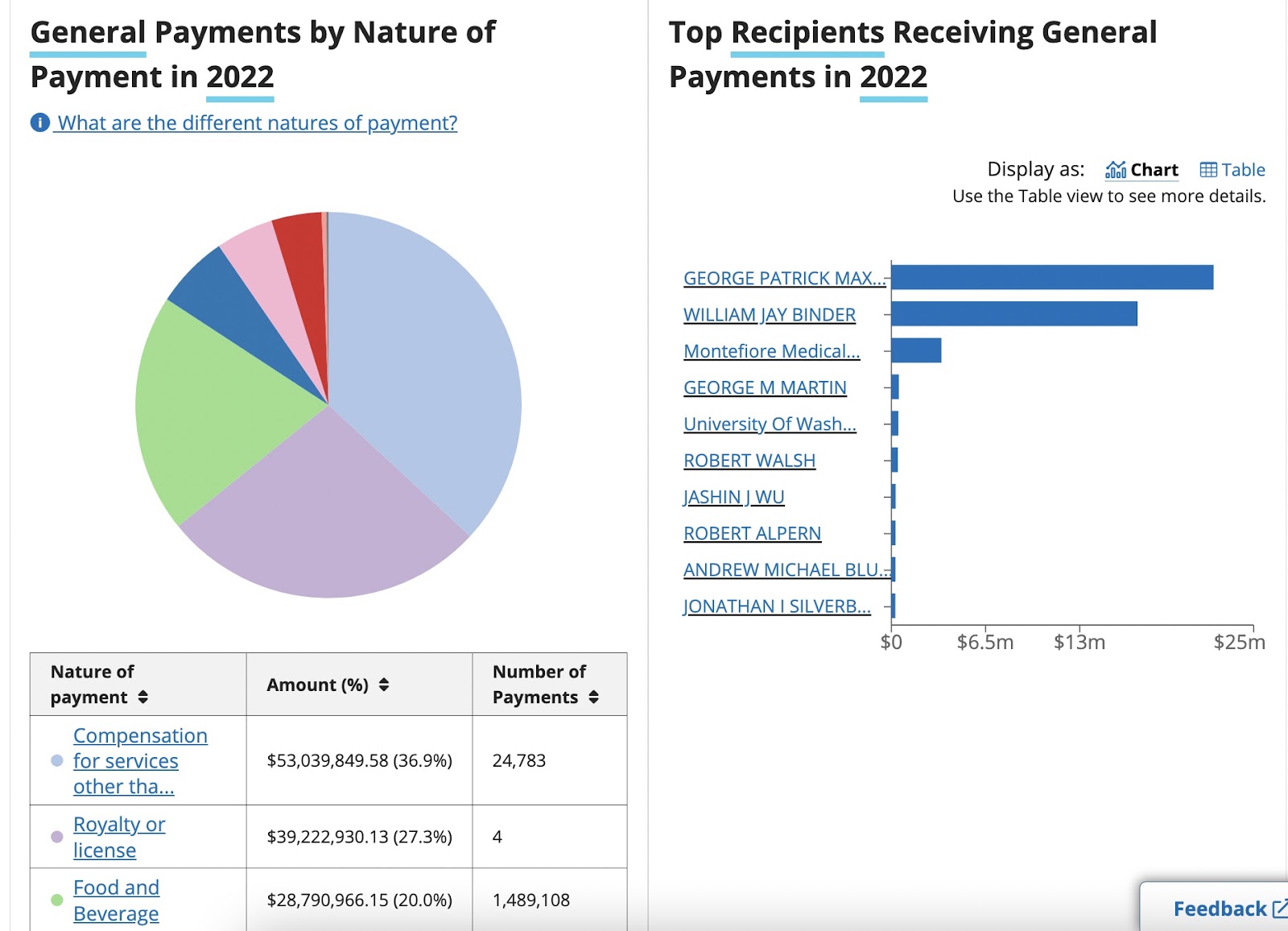
Abbvie payments breakdown openpaymentsdata.cms.gov.